Matters of the heart – Coronary Arterial Disease (Part I) : How heart’s already tough job becomes tougher
Introduction: There is no ‘hierarchy’ of importance of our organs; they are all equal, right? But then some are ‘more equal than others’. A kidney is donated, liver and brain are lobotomized (i.e. parts cut off and removed), limbs are amputated, blood is donated, bone marrow is transplanted, reproductive cells are extracted and stored, gall bladders are removed, uterus is excised, the prostate in men is ‘down-sized’ (benign) or removed altogether (malignant)…. and life goes on. But the heart must remain whole and healthy or the life becomes much less worth-living or, worse, is lost. Let’s see why.
This fist of an organ performs the most fundamental of life-sustaining tasks continuously – distributing blood all over the body and collecting it for fresh oxygenation. The whole body is its ‘territory’. This it does in the face of serious ‘situational’, pre-existing resistances to its performance despite nature’s best ‘design’. Age adds its own spanners in its works. When today’s life and what we do with it further loads it, it protests and, if it is neglected, simply gives up.
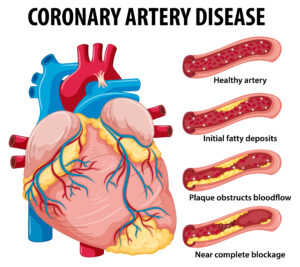 Diseases of the heart and blood vessels (cardio-vascular) are many but the most rampant, insidious and secular one is the Coronary Arterial Disease (CAD) and its after-effects – the single largest killer worldwide. It is the partial or full blockage (occlusion) of the artery that supplies blood to the heart itself, obviously enabling the heart to function. Ironically, all the associated words like angina, chest-pain, blood pressure, hypertension, heart attack, cholesterol… keep flying in the air. Some of us blithely keep mouthing even scarier ones like atherosclerosis, angioplasty, angiography, coronary bypass graft, heart transplant, myocardial infarction etc. But the common refrain is: “It can’t happen to me”. What can we call these, seeing blind and hearing deaf?! Schizophrenics, perhaps.
Diseases of the heart and blood vessels (cardio-vascular) are many but the most rampant, insidious and secular one is the Coronary Arterial Disease (CAD) and its after-effects – the single largest killer worldwide. It is the partial or full blockage (occlusion) of the artery that supplies blood to the heart itself, obviously enabling the heart to function. Ironically, all the associated words like angina, chest-pain, blood pressure, hypertension, heart attack, cholesterol… keep flying in the air. Some of us blithely keep mouthing even scarier ones like atherosclerosis, angioplasty, angiography, coronary bypass graft, heart transplant, myocardial infarction etc. But the common refrain is: “It can’t happen to me”. What can we call these, seeing blind and hearing deaf?! Schizophrenics, perhaps.
The idea behind this post is to understand (i) the working of the heart and its already significant routine load, (ii) how a creeping abnormality can, if undetected or ignored, add to it with serious consequences and (iii) how common sense, science and technology can be modeled to demystify most heart-related issues. It is hoped that this will help us understand CAD and its downstream effects better, reduce its incidence and cope with it more effectively.
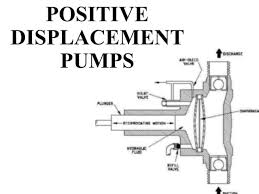 We start with the ‘model’ of a positive displacement pump (one that applies direct force to the liquid as in a pulsating liquid-filled balloon) circulating water in an elaborate piping system. In the next post, we deal with actual disease conditions. A hardworking attempt has been made to simplify a complex organ and the systems around it. As a lightening touch, let’s begin this post with a humourous heart and tongue-in-cheek, but the brain at its best.
We start with the ‘model’ of a positive displacement pump (one that applies direct force to the liquid as in a pulsating liquid-filled balloon) circulating water in an elaborate piping system. In the next post, we deal with actual disease conditions. A hardworking attempt has been made to simplify a complex organ and the systems around it. As a lightening touch, let’s begin this post with a humourous heart and tongue-in-cheek, but the brain at its best.
Medical science, ‘C’ and confusion!: I took inordinately long to figure out that CAD is Coronary Arterial Disease, CHD is Coronary Heart Disease but CVD is Cardio Vascular Disease. I did eventually figure out for my own consumption, that CAD leads to CHD and, both together, are a large part of CVD but not without cursing them for such compulsive commitment to ‘C’. But the medical science was not done confusing; a highly related cluster of disease conditions – cerebro-vascular diseases, stemming from impaired supply of blood to the brain (cerebrum) – has to stay cerebro-vascular; CVD has already been occupied, remember?! In reality, however, CVD encompasses cerebrovsacular.
Here’s a cample, sorry, sample of ‘C’ words:
Cerebrum, Cerebellum, Cranium, Concussion, Chiasma, Cornea, Cochlea, Canal, Cartilage, Clavicle, Column, Cilia, Collar, Cell, Cyst, Cuticle, Cutaneous, Co-enzyme, Cataract, Cavity, Cardiac, Coronary, Cortex, Cholesterol, Cesarean, Cervix, Curetting, Cecum, Cirrhosis, Chylomicrons, Colon, Chyme, Chyle, Capsule, Cholera, Colitis, Cancer, Corona………. See?
Now, cardium in the mouth, let’s delve seriously into the matters of the heart.
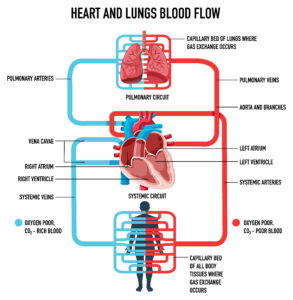
The load of the elaborate blood circulation scheme around the heart: Our heart is roughly in the top 1/5 of our body and must distribute blood all over it. Let’s try and grasp the overall enormity of this life-sustaining task given the distribution of our body around it.
- Pumping out blood to all parts of the body beginning with itself (i.e. the wall; it’s a hollow organ) thru the coronary artery and ensuring that it reaches every cell of every tissue of every organ.
- Retrieving the ‘spent blood’, and pumping it out to the lungs for oxygenation (refer Post15: OXYGEN, FOOD AND LIFE : PART I (HOW OXYGEN MEDIATES IN LIFE AND FOOD PROCESSING).
- Ensuring disposal of all non-fecal waste products.
- Receiving oxygenated blood from the lungs and pumping it out all over again as in 1 above. And do this some 70 – 80 times a minute, every minute of the life itself.
- Adjust itself, often in tandem with the lungs, for exercise, rest, sleep, eating, aging, pregnancy, disease, anxiety and similar emotions, etc. Some things look easy, especially if they keep working seemingly effortlessly, but aren’t. Driving up the US East Coast from Miami to Boston in December is tough even if you have the best car and you are a damn good driver.
So ‘have a heart’ and take care of it.
Adapted mechanics of pump-driven flow of water in a pipe: A water circulation scheme powered by a pulsating or receiprocating pump is an amazing ‘model’ to explain heart’s job:
 Even in a smooth, uniform, straight, horizontal pipe, energy is wasted in overcoming water’s own inherent resistance to flow (viscosity) and some nominal ‘friction’ at its contact with the inner surface of the pipe.
Even in a smooth, uniform, straight, horizontal pipe, energy is wasted in overcoming water’s own inherent resistance to flow (viscosity) and some nominal ‘friction’ at its contact with the inner surface of the pipe.- We know, from experience and commonsense, that the ‘flow rate’ at all points has to be the same otherwise there would be accumulation at some points and depletion at the others. Thus the kinetic energy of the water is constant.
- If the pipe reduces in diameter, the water will flow with greater speed i.e. kinetic energy will increase but, since energy can neither be destroyed nor created, this increase will come at the cost of its ‘pressure energy’ i.e. its pressure will drop. From this and 1 above, there is always a pressure drop when a liquid flows.
 The potential energy of water increases if the pipe slants or bends upwards; this increase can come only at the cost of increased ‘strain’ to the pump if the pump is physically pushing the water as with a piston.
The potential energy of water increases if the pipe slants or bends upwards; this increase can come only at the cost of increased ‘strain’ to the pump if the pump is physically pushing the water as with a piston.- Whenever the flow takes a turn or bifurcates, there is flow disturbance which adds to the ‘pressure drop’.
- Friction, height increases and decreases, bends, U turns, bifurcations etc. are real and hence pressure drops must always be expected. The pump mobilizing the water must account for them.
- A non-return valve in the pipe will allow water to flow only in the direction of flow; the reversal will be stopped by automatic closure – often by past-the-valve water itself. It is inherently ‘on-off’ i.e. it will be either fully open or fully closed and will allow water to flow at full flow or stop it altogether.
- You know that even clear-looking wind brings in fine dust that we find spread like a thin covering on horizontal surfaces at home. You have also experienced the gradual scaling of pipes carrying supposedly clear water. These are the symptoms of a fluid ‘shedding’ its suspended particles when its velocity (speed or direction or both) changes. At any ‘flow disturbance’, such insolubles separate out because water’s momentum is disturbed. Bends, U-turns, T-joints, bifurcations, even functional pipe fittings are a potential site for such settling or ‘scaling’. The smaller the pipe and lower the flow rate, the more the susceptibility to blockage.
- A constriction in the pipe in the form of a water-insoluble deposit will change the flow pattern on both sides of the constriction which will come at the cost of a ‘pressure drop’. In a way, the rise of the pressure before the constriction is the instinctive response to maintain the flow rate despite the disturbance. Since the industrial pipes are quite rigid, they cannot be dilated at the scaling nor, usually, poked; the pipe has to be ‘descaled’- one of engineers’ routine tasks when the plant is shut down. (Of course, our body cannot be ‘shut down!). Or the scaled blockage has to be bypassed by additional external piping. Or that pipe-length changed. All very simple and real.
- If a large scale-deposit in piping suddenly comes loose in a narrow pipe, say, because of vigorous tapping or sudden scale-rubbing flow, the released debris can block the pipe at the nearest bend.
- In a ‘positive displacement’ pump, a piston or a diaphragm or a flexible pouch sends the water rushing out by applying direct force. Any obstructions in the pipe and each of its branching, size reduction, etc. will strain the pump to sustain the flow.
- If the delivery side of the pump has two branches and the smaller of them is constricted, (i) the flow of water and its pressure downstream of the constriction will reduce, (ii) the pressure upstream of the constriction and also in the unconstricted branch will increase.
 If a clean branch on the delivery side of the pump is completely closed far away from the pump by closing a valve there (as in a tight cuff just above your elbow), the flow in that branch will stop. The pressure in that branch up to the valve will be the delivery pressure of the pump which will also prevail in all unclosed branches. You get a hint of what that frightening constriction on your biceps is doing when your ‘bp’ is being measured, right?
If a clean branch on the delivery side of the pump is completely closed far away from the pump by closing a valve there (as in a tight cuff just above your elbow), the flow in that branch will stop. The pressure in that branch up to the valve will be the delivery pressure of the pump which will also prevail in all unclosed branches. You get a hint of what that frightening constriction on your biceps is doing when your ‘bp’ is being measured, right?
(Leonardo da Vinci is reported to have said: Simplicity is the ultimate sophistication. Hope this simplification-cum-modeling is sophisticated enough.)
 Water-pipe-pump vs. blood-vessel-heart: I can’t think of a more complex natural liquid than the blood despite water being its most dominant component! (Milk would be a close second.) It flows as a liquid in our body but can gel up to stop flowing when it comes out thru a wound! It contains dissolved, un-ionized organics (glucose, urea, glycerol), ionized solids (NaCl), proteins, protein-fat complexes (cholesterol), fatty acids, fats, amino acids, dissolved gases, millions of diverse live cells, invading foreign particles and pathogens, antibodies….. If you want to fathom nature’s ability to simplify thru complexity, look no further than the blood! Leonardo is probably frowning his displeasure in his grave.
Water-pipe-pump vs. blood-vessel-heart: I can’t think of a more complex natural liquid than the blood despite water being its most dominant component! (Milk would be a close second.) It flows as a liquid in our body but can gel up to stop flowing when it comes out thru a wound! It contains dissolved, un-ionized organics (glucose, urea, glycerol), ionized solids (NaCl), proteins, protein-fat complexes (cholesterol), fatty acids, fats, amino acids, dissolved gases, millions of diverse live cells, invading foreign particles and pathogens, antibodies….. If you want to fathom nature’s ability to simplify thru complexity, look no further than the blood! Leonardo is probably frowning his displeasure in his grave.
Important: (i) Blood cells are obviously not dissolved and hence they can stick together (agglutinate) to from a clump. (ii) A clot can form in flowing blood (the kind that stops your bleeding on the surface) if the inside lining of the blood vessel is injured. (iii) Fat – whether triglycerides, fatty acids or non-glyceride lipids like forms of cholesterols – is ‘dispersed’ in the blood thru chemical manipulation, not dissolved and hence can separate out if given a chance. Engineers call this possible ‘thermodynamic spontaneity’. (iv) These three are the commonest potential separations from the blood – chemists can liken them to ‘precipitates’. Chemical Engineers will struggle to decide if this is ‘multi-phase’ flow. Honestly, I don’t know. (v) Blood in a metal pipe and water in blood vessels are ‘loaded’ imaginary scenarios which may be never tried out!
The blood vessels couldn’t be more different from the practically rigid pipe; they have a detailed structure (‘histology’) containing muscle fibers that give them flexibility and an inner lining (endothelium). But a lot like blood-water duo, they would experience similar stresses like pipes despite being able to dilate a little. Ironically, a positive displacement diaphragm pump and the heart are closest in form and function; only we can easily get a new pump or pipe but……..!
 Heart’s ‘circumstances’ as it performs: Our heart is an exceedingly complex positive displacement pump with four chambers and non-return valves for chamber-chamber and chamber-blood vessel transfers. We will focus only on its left ventricle that sends blood rushing out past a non-return aortic valve into the aorta – body’s largest blood vessel supplying nourishing, oxygenated blood to every nook and corner of the body. (Ref post 15, OXYGEN, FOOD AND LIFE : PART I (HOW OXYGEN MEDIATES IN LIFE AND FOOD PROCESSING). We will demystify ‘blood pressure’ in the next post.) Actually it can be about an inch in diameter at its widest (all your domestic plumbing – gas and water – is only a fraction of that) and be over a foot long; it can’t get blocked easily because of sheer size.
Heart’s ‘circumstances’ as it performs: Our heart is an exceedingly complex positive displacement pump with four chambers and non-return valves for chamber-chamber and chamber-blood vessel transfers. We will focus only on its left ventricle that sends blood rushing out past a non-return aortic valve into the aorta – body’s largest blood vessel supplying nourishing, oxygenated blood to every nook and corner of the body. (Ref post 15, OXYGEN, FOOD AND LIFE : PART I (HOW OXYGEN MEDIATES IN LIFE AND FOOD PROCESSING). We will demystify ‘blood pressure’ in the next post.) Actually it can be about an inch in diameter at its widest (all your domestic plumbing – gas and water – is only a fraction of that) and be over a foot long; it can’t get blocked easily because of sheer size.
As blood rushes out into the aorta past a non-return valve, it is at systolic pressure. Note that the pressure within the left ventricle per se’ would be very minutely greater because of the miniscule resistance of even the open NRV and this would be the ‘pressure drop’ of the NRV. The aorta immediately starts branching (buckling down to its task) and its first branch is the coronary artery, so called because it is at the corona (top) of the heart. It has to supply blood to the entire heart wall or myocardium. Since heart is a fist-like organ, the coronary has to ‘arch’ over the heart top and branch further before diving into the myocardium to cover the whole of the heart.
After the coronary branch, the aorta further branches, sending one major branch upwards and one downwards to cover the body. Note how these heart-straining convolutions are inevitable and have to be taken in its stride by the heart. Profuse branching into progressively smaller and smaller vessels carries the blood everywhere in the body, the brain included. At the nutrition and oxygen delivery sites, they have to diffuse out of the minute capillaries and into the consuming cells. This transfer across a ‘resistance’ is because of our ‘blood pressure’!
The capillaries then progressively regroup (ref post 15 again) to become large veins returning blood. Just imagine the sheer ‘resistance to blood flow’ that the heart has to endure because branches, branches to branches, twists and turns, long distances, diffusion resistances….. from its perch in the upper chest. Beach running with a 25 kg load would be an experiential example. Or swimming a km against the flow of a river in spate. You probably can’t do either but your heart has been uncomplainingly laboring away since your birth. Don’t give it reasons to complain!
In the next post, we will see how blockages develop in the coronary artery or its branches and what they do to the heart itself and the rest of the body. True to our tradition, we will highlight the role of food in causing this and, more importantly, remedying it – inevitably with lifestyle changes.
Next Post:
Matters of the heart, Coronary Arterial Disease: Part II
How it happens and how food and lifestyle can help
Visit disclaimer
7 thoughts on “Matters of the heart – Coronary Arterial Disease (Part I) : How heart’s already tough job becomes tougher”
Thanks for the sensible critique. Me & my neighbor were just preparing to do a little research on this. We got a grab a book from our area library but I think I learned more from this post. I’m very glad to see such excellent info being shared freely out there.
Dear Sir/ma,
We are a financial services and advisory company mandated by our investors to seek business opportunities and projects for possible funding and debt capital financing.
Please note that our investors are from the Gulf region. They intend to invest in viable business ventures or projects that you are currently executing or intend to embark upon as a means of expanding your (their) global portfolio.
We are eager to have more discussions on this subject in any way you believe suitable.
Please contact me on my direct email: ahmed.abdulla@dejlaconsulting.com
Looking forward to working with you.
Yours faithfully,
Ahmed Abdulla
financial advisor
Dejla Consulting LLC
Sir,
Email sent to you on your suggested e-mail id.
Regards.
Hi my loved one! I wish to say that this post is amazing, great written and include approximately all significant infos. I’d like to see extra posts like this .
Nice read, I just passed this onto a colleague who was doing some research on that. And he just bought me lunch as I found it for him smile Therefore let me rephrase that: Thanks for lunch! “We have two ears and only one tongue in order that we may hear more and speak less.” by Laertius Diogenes.
Great post. I am facing a couple of these problems.
I believe you have mentioned some very interesting points, thanks for the post.