Diabetes – the creeping, corrosive curse (But food, lifestyle and even attitude can help!)
(This post became large as it needed to be coherent and complete; do stay with it).
We saw obesity as a rampant chronic condition that creeps up on us thru a series of factors and is measurably reflected in our BMI. (Ref. post 21, Obesity and food – accumulation of the unused: Part I, Understanding obesity). Diabetes is strikingly similar though it creeps in invisibly and is measured only thru analysis. A staggering close to 11 % of world’s adult population is diabetic with promise of steady, inevitable increase. Like obesity, it gnaws at every organ and system in the body and burdens life with a slew of somewhat vaguely defined and felt symptoms.
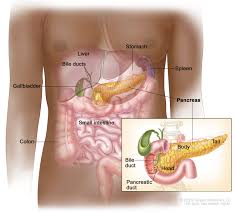
What is diabetes: It is a chronic hormonal-metabolic disorder characterized by raised blood glucose levels, mediated by insufficient insulin action. Such ‘lack of action’ can be because of insufficient quantity of insulin (Type I) or insufficient effectiveness of adequate quantity (Type II). Insulin is a hormone – all hormones are, by definition, secreted directly into the blood stream by the so-called ductless or endocrine glands. In this case, pancreas is that endocrine gland and, given the wide prevalence of diabetes, the disease ‘enjoys’ the king’s status in the field of endocrinology. Interestingly, pancreas also produces ‘pancreatic juice’ which it sends to the small intestine to help in digestion thru a duct and hence, in that sense, it is not ductless! Such complexity packs mind-boggling functionalities in our small frame making life itself happen.

Its most outward symptoms are frequent thirst, excessive urination urge and a feeling of fatigue and delayed healing of cuts, bruises and boils; deep down, it subliminally affects many of our organs and systems. Disconcertingly, it cannot be cured; at the most detected in time and reversed to a safe status and managed. But well-managed diabetes allows a good enough quality of life, barring the bitterness of having to stay away from sweets.
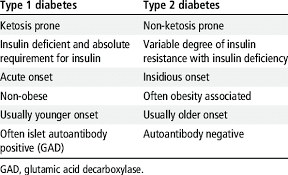
Types and causes: As we have noted in an earlier post, insulin mediates in ensuring that glucose in the blood crosses the walls or outer-most membranes of the cells. It is thus the ‘escort’ to glucose into the cells where it is bio-combusted to release energy. (Post 15, Oxygen, food and life: Part I, How oxygen mediates in life and food processing). When insulin level is inadequate in relation to glucose or the cells resist the efforts of insulin to escort glucose into cells, glucose tends to linger in the blood raising its levels. The former condition is ‘insulin deficiency’ and the latter, insulin ‘resistance’ or ‘insensitivity’.
Insulin-dependent Diabetes Mellitus (IDDM) – also called Type I diabetes – is caused by impaired production of insulin by the specialized cells in the pancreas. Sometimes called ‘juvenile diabetes’ because it strikes early; it is a lot rarer than the ‘main type’. Insulin replacement or shots are the standard treatment.
Non-Insulin-Dependent Diabetes Mellitus (NIDDM) – also called Type II diabetes – sneaks in later in life. It is Type IIa when the patient is lean, Type IIb when obese which is a lot more common. Type II diabetes is a lot more common than type I (rough ratio, 9:1) and, generally does not require insulin doses. India has world’s largest population of diabetes patients – about 10 % of our large population – and it is spreading at an alarming rate.
A review of nutritive carbohydrates vis a vis diabetes: (Ref post 2, Health, happiness, life and food: Part I – What are they? and posts 21, 22, 23, 24 on Obesity). ‘Nutritive carbohydrates’ are so called because they do get digested, absorbed into the blood and provide energy to do everything we do with provision for storage for ‘the rainy day’. This is a vast world, ubiquitous in the plant kingdom, which can be treated as a few ‘classes’ relevant to human life. A brief review:
Starch and cellulose (along with hemicelluloses whose molecular structure includes non-glucose monomers also and is branched and smaller than cellulose) are polysaccharides. Only starch is ‘nutritive’ as you know from the referred posts. Oligosaccharides result from limited hydrolysis (chemical or enzymatic) of starch and are formed as an ‘intermediate’ transient product during starch digestion. Sucrose (table sugar), Maltose and Lactose are the main disaccharides consisting of chemically bonded monosaccharides which are the simplest sugars that our body can utilize.
Starch is a general, umbrella name given to polymers of glucose i.e. each starch molecule consists of many glucose units chemically bonded together. Grains, legumes (daals), beans, kathols, potatoes and other tubers are the main sources of starch.
The molecular structure based classification of starches: Natural starch is straight-chain (amylose) or branched (amylopectin) and both types exist together in different proportions giving all natural starches the primary differentiator in character. The straight portions of amylopectin and the entire chains of amylose have glucose-glucose linkages that are different from the linkages where branches emanate in amylopectin. When forcibly chemically hydrolysed, they both produce glucose.
In the small intestine, pancreatic amylase breaks down amylose gradually under the action of pancreatic amylase detaching glucose units at the ends and cleaving the chain at intervals producing ‘oligosaccharides’.
Amylopectin similarly hydrolyses or digests but faster than amylose because its branched, less stretched structure facilitates the catalytic action of enzymes. However, it cannot break the different type of glucose-glucose linkages at the spots where branches originate where its action stops. Pancreatic amylase, therefore, produces glucose and small chains (that were earlier branches) called ‘limit dextrins’. These are immediately taken up by intestinal enzymes (distinct from pancreatic enzyme) which complete the task of breaking natural starch into glucose. Amylose and amylopectin thus disappear to produce glucose which has the right molecular size to easily be absorbed into the blood stream. This is obviously, the onset of a ‘glucose spike’ which has thankfully come after a lapse of time since eating because of the elaborate and time-consuming digestion process.
 After the meal, the simpler sugars have earlier been absorbed into the blood and started producing bio-energy (ref posts on obesity) thereby first raising and then lowering the blood glucose levels. (Note how this makes the unwelcome physical exertion necessary!). Thus a sweet dish (e.g. suji halwa or sheera) with dominating disaccharide of sugar must be eaten in moderation to lower the quick-happening glucose spike which will be flowed by a somewhat mellow (or flattish) rise because of disappearing starch. Extremely unadvisable to have a large serving of such a halwa late at night, even for non-diabetics. Ditto: midnight fridge raids for ice-cream and chocolate. The problem is: you don’t collapse, so there is no immediate deterrent; it ‘grows’ corrosively on you.
After the meal, the simpler sugars have earlier been absorbed into the blood and started producing bio-energy (ref posts on obesity) thereby first raising and then lowering the blood glucose levels. (Note how this makes the unwelcome physical exertion necessary!). Thus a sweet dish (e.g. suji halwa or sheera) with dominating disaccharide of sugar must be eaten in moderation to lower the quick-happening glucose spike which will be flowed by a somewhat mellow (or flattish) rise because of disappearing starch. Extremely unadvisable to have a large serving of such a halwa late at night, even for non-diabetics. Ditto: midnight fridge raids for ice-cream and chocolate. The problem is: you don’t collapse, so there is no immediate deterrent; it ‘grows’ corrosively on you.
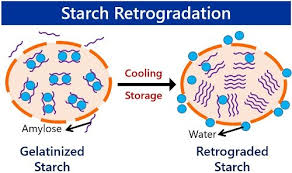 When rice, potatoes, wheat flour (and refined flour), millets, legumes or daals, beans etc are cooked in water, the polymeric chains get loosely physically connected thru bridges of water molecules. This is the classical ‘gelation’ or gel formation – gel is a liquid trapped in a solid – and the process is called gelatinization of starch. Gelatinized starch, obviously not natural, is fluffier, soft and a bit transluscent; now you know what happens when rice becomes ‘bhaat’. This actually improves digestibility – one of the functions of cooking. However, the trapped water gradually oozes out of the gel on cooling and storage, bringing the chains forcibly closer and causing them to coil up a bit. This is the retrograded starch which is more compact and harder than gelatinized starch and less digestible and hence is classified as resistant starch.
When rice, potatoes, wheat flour (and refined flour), millets, legumes or daals, beans etc are cooked in water, the polymeric chains get loosely physically connected thru bridges of water molecules. This is the classical ‘gelation’ or gel formation – gel is a liquid trapped in a solid – and the process is called gelatinization of starch. Gelatinized starch, obviously not natural, is fluffier, soft and a bit transluscent; now you know what happens when rice becomes ‘bhaat’. This actually improves digestibility – one of the functions of cooking. However, the trapped water gradually oozes out of the gel on cooling and storage, bringing the chains forcibly closer and causing them to coil up a bit. This is the retrograded starch which is more compact and harder than gelatinized starch and less digestible and hence is classified as resistant starch.
 Leftover rice stored in the fridge, resists digestion in the small intestine when eaten next morning. Since it must ‘move on’ after its designated time there, it enters the colon or the large intestine partly intact. This obviously limits its ‘glucose spike’ and, fortuitously, it is taken up by the colonic microbiome to do some favorable things. This gives it the status of a prebiotic. (Ref post 2: Health, happiness. life and food). We Trivedi’s sometimes make simple breakfast using leftover rice mixed with boiled rajma (kidney beans/chhole (bold ckickpea)/peas/soya nuggets. It makes a proteinaceous, low glycemic breakfast with minimal fuss. Whenever we cook rajma or chhole, we ensure some surplus of the boiled form. It also makes excellent patties with any cooked starchy food (rice, potatoes, bread crumbs) and suji (semolina) – a great breakfast. It is amazing what you can do with just a bit of planning and foresight.
Leftover rice stored in the fridge, resists digestion in the small intestine when eaten next morning. Since it must ‘move on’ after its designated time there, it enters the colon or the large intestine partly intact. This obviously limits its ‘glucose spike’ and, fortuitously, it is taken up by the colonic microbiome to do some favorable things. This gives it the status of a prebiotic. (Ref post 2: Health, happiness. life and food). We Trivedi’s sometimes make simple breakfast using leftover rice mixed with boiled rajma (kidney beans/chhole (bold ckickpea)/peas/soya nuggets. It makes a proteinaceous, low glycemic breakfast with minimal fuss. Whenever we cook rajma or chhole, we ensure some surplus of the boiled form. It also makes excellent patties with any cooked starchy food (rice, potatoes, bread crumbs) and suji (semolina) – a great breakfast. It is amazing what you can do with just a bit of planning and foresight.
 Though resistant retrograded starch results from mundane cooking and storage, it is still not natural starch. Cross-linked starch is chemically modified starch where new chemical bonds are created by an industrial process across glucose polymeric chains. These are durable bonds unlike water bridges in gelatinized starch and hence cross-linked starch is strongly resistant starch. It is used to make some diabetic formulations.
Though resistant retrograded starch results from mundane cooking and storage, it is still not natural starch. Cross-linked starch is chemically modified starch where new chemical bonds are created by an industrial process across glucose polymeric chains. These are durable bonds unlike water bridges in gelatinized starch and hence cross-linked starch is strongly resistant starch. It is used to make some diabetic formulations.
When grains or legumes or beans are ground coarse and not excessively cooked, some of the starch in them remains covered with non-digestible plant cell structures (mainly cellulosic cell walls) which limits its digestion. This is a form of natural resistant starch. Porridges and savory spoonable dishes prepared from what are popularly called ‘dhalia’ or ‘dalia’ are, therefore, great breakfasts. Broken rice, wheat dahlia, oats dhallia, rolled oats and barley and coarsely ground corn, pearl millet (bajra) and sorghum (jowar) are good breakfast starters.
Obviously, then, the digestibility of a starch determines how much glucose (and how fast) is sent into the blood stream, embedded in the digestive tract. This is a strong determinant of how much of an enemy it is of a diabetic. Note that digestibility is a strong function of the starch molecular structure, as expected. Coarse grain starch is resistant despite being natural. Note how reduced processing (limited grinding) is helpful here. We have already made a strong case for reducing processing in earlier posts.
We have already seen in the Obesity posts (nos. 21 to 24) that surplus glucose is stored in the liver as glycogen (also called ‘animal starch’) which is a branched glucose polymer and insoluble in water. Vegetarian food provides no glycogen. Its existence in human bodies makes it convenient to exclude it from classification of starches as a component of what we eat. Obviously, digestibility – a direct function of the molecular structure – is a great basis for such a classification.
Sucrose, our good old sugar, is a disaccharide of glucose and fructose. We have already seen in earlier posts that fructose is converted to glucose in the liver and hence sucrose raises the blood glucose level slower than equivalent amount of glucose.
Lactose or milk sugar is a glucose-galactose disaccharide unique to milk.
Maltose is a glucose-glucose disaccharide that is produced when starch is digested before it further breaks into glucose. Processed foods containing oligosaccharides and maltose are sometimes called ‘malted’ foods.
Fructose (a part of daily sugar molecule) and galactose (a part of milk sugar or lactose) are monosaccharides and close cousins of glucose and have the same molecular formula; they have minor differences in detailed structure which make them behave differently from glucose. In the body they all eventually become glucose and join the energy release metabolism.
Glucose is the ultimate simple sugar, a monosaccharide and energy molecule that all carbohydrates have to become in our body. It rides in the watery part of the blood totally dissolved except a tiny part attached to haemoglobin which is an iron-protein complex. It resembles urea in being dissolved without ionization and is unlike NaCl which is ionized. This dissolved status of glucose is readily available to tissues into which it diffuses to get combusted to release energy. Obviously, there is no question of glucose being ‘thrown out’ of blood and parking itself on the inner walls, like cholesterol.
The most important point of this discussion is: nutritive carbohydrates are a ‘spectrum’ that inject glucose into the blood at different rates and at different stages during the digestion cycle. Obviously, limit simple sugars; adopt complex ones more.
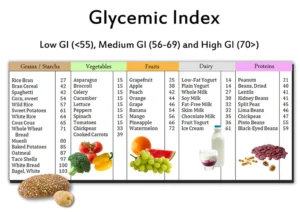
The essence of Glycemic Index (GI): It is an indicator of how fast a food will raise the blood glucose level i.e. essentially, how fast its carbohydrates become glucose in the blood stream. The ‘size of the rise’ per se’ for a fixed quantity of food is encapsulated in ‘Glycemic Load’ which reflects the concentration or level of glucose-releasing carbohydrates. Obviously, we need to consume low GI-low GL foods consistent with our BMI, hereditary and physical activity levels so that smaller amount of glucose enters the blood slowly and whatever enters is consumed for energy. It helps that the beneficial daals, beans, cereals, millets, kathols and nuts, essential as protein sources in vegetarian diet, are actually low in both GI and GL while they work their non-glucose wonders.
Glucose, which instantaneously enters the blood stream on being ingested has been arbitrarily assigned a GI of 100. Our daily table sugar (i.e. sucrose) has a GI of 65. Interestingly, fructose, a part of sucrose, has a low GI of about 25 though it is the sweetest among dietary carbohydrates. In fact, the GI of sugar is pulled down by fructose. Fructose raises glucose level slowly and should be everybody’s darling as a sweetener. But beware: fructose has been indicted in many conditions including cancers. Thank God, our good old chemical soldier – the liver – converts it into glucose.
Note: How quickly after eating, glucose from a food will enter the blood and raise its level is reflected in GI, how much glucose (per unit weight) will enter the blood is reflected in GL but the pattern of rise with time [mathematically, the rise as a function of time or dS/dt as f(t)] will also depend on your physical activity level. (Ref post 22, Obesity and food – accumulation of the unused: Part II, Details of how the food-obesity linkage plays out.)
If you gobble up a few tablespoonfuls of glucose at midnight before quickly going to sleep, the effect will be a spike in glucose level. If you chew up an equivalent quantity of oats and start exercising, there will be an unnoticeable glucose spike, even none at all, because the slowly entering glucose will be combusted as it enters. Oats have lower GI as well as GL; reason why oats have struck roots in India in 10 years unlike cornflakes which are struggling 30 years after entering.
Concurrent and eventual effects of diabetes: While Type IIb patients have to face the double whammy of diabetes and obesity, Type IIa patients have it relatively easy. But the Type I patients still have to contend with the prospect of glucose-mediated atherosclerosis.
This apart, diabetes affects almost all our systems, of particular concern is ‘diabetic retinopathy’ which severally affects the retina in the eye and diabetic nephropathy which affects kidney’s efficiency. Diabetic neuropathy affects nerves leading to tingling sensation on the skin for starters.
 Complex carbohydrates: These are essentially a cluster of digestible glucose polymers (amylose and amylopectin) and insoluble and soluble fiber in natural foods (ref post 2). Foods carrying them (daals or lentils, legumes or kathol, beans, cereals – especially oats and barley, millets, chia seeds, quinoa etc) have low GI and low GL and also offer benefits of proteins and dietary fiber. They are considered the frontline of dietary, non-medicine defense against and management of diabetes.
Complex carbohydrates: These are essentially a cluster of digestible glucose polymers (amylose and amylopectin) and insoluble and soluble fiber in natural foods (ref post 2). Foods carrying them (daals or lentils, legumes or kathol, beans, cereals – especially oats and barley, millets, chia seeds, quinoa etc) have low GI and low GL and also offer benefits of proteins and dietary fiber. They are considered the frontline of dietary, non-medicine defense against and management of diabetes.
 Empty calories: Everything sweet – sweets, tea, coffee, chocolate, ice-cream, aerated drinks, fruits and their juices, jams and jellies, etc. – carry sugar and other calorie-contributing constituents. When a food product provides mainly calories and little ‘collateral’ benefit, they are called ‘empty calories’. Sugar, aerated drinks, toffees are typical examples. Sweets, ice-creams, biscuits and chocolates are examples of ‘fun foods’ that have high GI and GL but offer moderate other benefits, e.g. chocolates bring in antioxidants and, for physically active young people, ice-cream is a calorie-dense multifaceted food.
Empty calories: Everything sweet – sweets, tea, coffee, chocolate, ice-cream, aerated drinks, fruits and their juices, jams and jellies, etc. – carry sugar and other calorie-contributing constituents. When a food product provides mainly calories and little ‘collateral’ benefit, they are called ‘empty calories’. Sugar, aerated drinks, toffees are typical examples. Sweets, ice-creams, biscuits and chocolates are examples of ‘fun foods’ that have high GI and GL but offer moderate other benefits, e.g. chocolates bring in antioxidants and, for physically active young people, ice-cream is a calorie-dense multifaceted food.
Oats porridge with nuts, carrot/lauki halwa and French Fried Toast are examples of high GI high, GL foods with excellent collateral benefits. (Obviously, replacing sugar partly or fully with non-calorie, high intensity sweeteners will pull down both GI and GL in a graded way.) Chyavanpraash is unique in being high GI, low GL but, given its low consumption level, an excellent immunity booster at low glycemic cost. Some day, we will talk about a brilliantly special, highly differentiated variant of chyavanpraash with universal appeal. (Meet Preeti in ‘About us’.) Fruits are ok within limits of quantity and spread over the day; always prefer whole fruits over juices – especially the thin, clarified, sweetened ones. Do note, however, that the glycemic index is high because of simple sugars; ideally combine it with plain milk or curd to reduce the load. Generally, a ‘mattha’ made with a fruit (banana, pineapple, mango, sapota or chiku, berries), sugar, stevia, oats and curd is a great ‘bachelor breakfast’. We plan to eventually adopt it as summer dinner.



Interpretation of the common food advice to diabetics:
- Several small meals spread out in the day: Replace 2 – 3 durable glucose spikes with several smaller, flatter, fast diminishing increases while taking care of nutrition.
- Avoid large, frequent servings of sweets: Multiple glucose spikes result in sustained high glucose levels in the blood. Accompanying fats are the double whammy.
- Adopt millets, beans, vegetables, daals: Complex carbohydrates, proteins and dietary fiber; vegetables (except potato and the like) have a low glycemic cost.
- Adopt aerobic exercise: Burns up circulating blood glucose and lowers its level and gradually lowers insulin resistance. Collateral benefits: makes you feel good, reduces obesity, increases hdl-cholesterol, strengthens heart and lungs, improves muscle tone.
- Avoid excessive fats and oils: Minimizes hyperlipidemia and obesity which promote insulin resistance.
- Stay cheerful and socially active: Frequent bouts of anxiety and similar feelings raise blood pressure (and may help cause atherosclerosis) leading to a series of serious chronic conditions. They also distort body’s overall hormone balance and suppress insulin production.
Life’s beautiful; don’t kill the goose laying golden eggs.
Next Post:
Dealing with diabetes thru diet
Avoiding, stalling, reversing and living with diabetes using food
Visit Disclaimer
11 thoughts on “Diabetes – the creeping, corrosive curse (But food, lifestyle and even attitude can help!)”
I have recently started a site, the info you provide on this web site has helped me greatly. Thanks for all of your time & work.
Very interesting points you have mentioned, appreciate it for posting. “A big man is one who makes us feel bigger when we are with him.” by John C. Maxwell.
I’ve been absent for some time, but now I remember why I used to love this website. Thanks, I’ll try and check back more frequently. How frequently you update your site?
Hi,
We update our website once or twice a month. You are welcome to subscribe to it to get an update whenever a new post drops. Stay tuned for more!
I like what you guys are up also. Such clever work and reporting! Carry on the excellent works guys I’ve incorporated you guys to my blogroll. I think it’ll improve the value of my site 🙂
Hiya, I’m really glad I’ve found this info. Today bloggers publish just about gossips and net and this is really annoying. A good blog with exciting content, that is what I need. Thanks for keeping this site, I will be visiting it. Do you do newsletters? Can’t find it.
Hi,
Thank you for the kind words. We don’t do newsletters, but you can subscribe to our blog to get regular updates about new posts that drop. Hope that helps.
Pretty section of content. I simply stumbled upon your website and in accession capital to claim that I acquire in fact loved account your blog posts. Anyway I will be subscribing in your feeds or even I success you get entry to persistently quickly.
Great perspective
I have been surfing on-line more than 3 hours as of late, yet I never found any interesting article like yours. It is beautiful value enough for me. In my view, if all webmasters and bloggers made just right content as you probably did, the net will be much more helpful than ever before.
he blog was how do i say it… relevant, finally something that helped me. Thanks