Blood pressure and hypertension – Their nature, origin, effects and remedies with focus on food
“I have BP”, has become a damning and, unfortunately, a common confession. Ironically, life is possible only because blood has pressure which sends the blood to the nooks and corners of the body. What we shouldn’t have is hypertension or excessive BP.
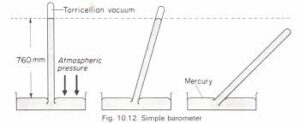
 What is pressure? It is the force exerted by a fluid (liquids and gases) per unit area of a surface at right angle to it. The atmosphere exerts a pressure on everything on the earth because of the collision of its particles with each other and the surfaces; we call it the ‘atmospheric pressure’. Quantitatively, it can typically support a 760 millimeter tall mercury column (varies nominally from place to place) when this pressure acts at the base of the column and the column has total vacuum at the sealed end. If it is a ‘U’ tube with the atmospheric pressure acting on one arm and the other arm connected to total vacuum, the difference in the heights of mercury in both the arms is the atmospheric pressure. ‘x mm of Hg’ is, thus, a unit of pressure.
What is pressure? It is the force exerted by a fluid (liquids and gases) per unit area of a surface at right angle to it. The atmosphere exerts a pressure on everything on the earth because of the collision of its particles with each other and the surfaces; we call it the ‘atmospheric pressure’. Quantitatively, it can typically support a 760 millimeter tall mercury column (varies nominally from place to place) when this pressure acts at the base of the column and the column has total vacuum at the sealed end. If it is a ‘U’ tube with the atmospheric pressure acting on one arm and the other arm connected to total vacuum, the difference in the heights of mercury in both the arms is the atmospheric pressure. ‘x mm of Hg’ is, thus, a unit of pressure.
 If your blood pressure is 120 mm of mercury, that is the height of the mercury column (with total vacuum over mercury in the sealed end) on the physician’s instrument (sphygmomanometer) that is supported by the air pressure in the cuff around your lower biceps when the tightness of the cuff has stopped blood flow. At this stage, the air pressure at the base of the mercury column in physician’s sphygmomanometer = the air pressure between the two layers of the cuff around your lower upper arm = the pressure of the blood stopped by the air in the cuff = the pressure of the blood delivered by the heart. (Ref post 25, Matters of the heart, Coronary Arterial Disease: Part I, How heart’s already tough job becomes tougher.)
If your blood pressure is 120 mm of mercury, that is the height of the mercury column (with total vacuum over mercury in the sealed end) on the physician’s instrument (sphygmomanometer) that is supported by the air pressure in the cuff around your lower biceps when the tightness of the cuff has stopped blood flow. At this stage, the air pressure at the base of the mercury column in physician’s sphygmomanometer = the air pressure between the two layers of the cuff around your lower upper arm = the pressure of the blood stopped by the air in the cuff = the pressure of the blood delivered by the heart. (Ref post 25, Matters of the heart, Coronary Arterial Disease: Part I, How heart’s already tough job becomes tougher.)
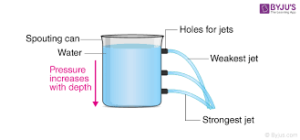
(All still liquids exert a ‘static’ pressure within its bulk and its value at any point in it is directly proportional to the depth. Flowing liquids also have pressure which gives them certain ‘pressure energy’ which is over and above the potential energy – because of the height from a reference point – and kinetic energy – because of its flowing speed. Your overhead water tank has maximum pressure at the bottom from where its distribution head emerges. Its value is maximum when the tank is full and you get water ‘with pressure’ in your taps. This translates to the maximum flow rate of water gushing out of your taps.)
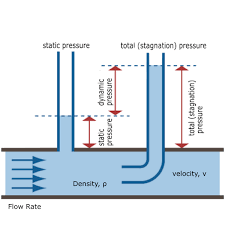
The moment a liquid flows, some of its pressure energy is converted to kinetic (flowing) energy and if its height increases, even potential energy, which come at the cost of the pressure energy. Here’s paying homage to Swiss physicist- mathematician Bernoulli who immortalized the concept of the total energy of a fluid remaining constant (under specified conditions) thru his celebrated Bernoulli’s Equation. Though it was essentially a version of the statement of the known conservation of energy, it ended up explaining a series of phenomena concerning fluid flow. (Ref above-mentioned post which also explains that some of the pressure goes into offsetting friction and flow pattern changes.)
What is ‘blood pressure’?: As the name suggests, it is simply the pressure that blood exerts against the walls of the blood vessels and the vessels, in return, exert on the blood. Now, pressure is nothing but ‘force per unit area’ and since the area is common, the mutual forces must also be equal. It is borne out by the observation that this ‘net zero’ force causes no displacement, in compliance of Newton’s law. There is however, some dilation (distortion) of the vessel which creates the ‘reaction pressure’ opposing the blood pressure.
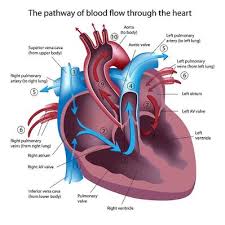

Systolic blood pressure is the pressure of the blood as it gushes out into the aorta with the contraction of the heart, actually its left ventricle. This exertion of force on the blood gives the systolic pressure the higher of the two well known values. Diastolic blood pressure is the residual pressure of the blood as the heart expands to its original size when the pumped blood is already ‘on its way’ into the aorta (and the coronary artery). At this stage, the aortic valve at the base of the aorta within the heart at the junction of the aorta and the left ventricle is closed. This is understandably lower than the systolic number but loaded with info on the condition of the aortic and coronary passages – especially the ‘cleanness’ and the flexibility. All high BP is worrisome but sustained high diastolic pressure is more so.
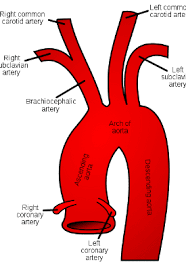
The arteries delivering blood all over the body have thicker walls and narrower lumens (the central axial hollow) than the veins taking blood back to the heart. Those close to the heart ( i.e. the aorta – the ‘delivery line of the heart’, the coronary artery and the pulmonary artery taking blood to the lungs for oxygenation from the heart) are designed elastic to ‘take’ the pulsating force exerted by the heart. (ref post 25). As the distance from the heart increases they become more ‘muscular’ i.e. with smooth muscles in their walls. In a young, healthy person, the blood vessel walls are supple and flexible because of healthy muscle fibers.
Note that the heart can do this ‘work’ because it receives nutrition and oxygen from the blood sent to its wall by itself! It knows how to take care of itself, doesn’t it, as long as you allow it to!
Cardiology, in its most basic form, is understanding why these pressure numbers are what they are, what they are doing to the heart and the rest of the body and how to ‘manage’ the ‘disturbances’ or ‘obstructions’ (of all types, not necessarily CAD origin) to maintain a semblance of smooth blood flow without tiring the heart excessively and depriving the myocardium and body tissues of oxygen and nutrition.
 Cardiac surgeons get rid of the ‘blockages’ in the blood vessels or dilate the vessels around the blockage in some way so that the effect of obstruction is decreased. Sometimes, they bypass them by creating a new loop for flow – a lot like the bypass on a stretch of road that is unusable. In extreme cases, they decide that the entire heart is past its ‘best before’ date and replace it with a relatively functional one extracted from a just expired donor.
Cardiac surgeons get rid of the ‘blockages’ in the blood vessels or dilate the vessels around the blockage in some way so that the effect of obstruction is decreased. Sometimes, they bypass them by creating a new loop for flow – a lot like the bypass on a stretch of road that is unusable. In extreme cases, they decide that the entire heart is past its ‘best before’ date and replace it with a relatively functional one extracted from a just expired donor.
Let’s salute the awesome capabilities of cardiac surgeons; what’s described here is simplified info meant as ‘information is power’. This is expected to ease the stress when it is likely to be at its worst.
 Measuring blood pressure: The physician ties his Sphygmomanometer cuff just above your left elbow – the level of your heart, for accuracy. In reality it can be done anywhere on the body when necessary. The tight grip of the cuff ensures that the air pressure in the cuff ‘balances’ the pressure of the blood in the blood vessels below your skin. The first time can be scary with the vice-like grip of the cuff and the doctor usually takes a couple of more readings when you are supposedly ‘relaxed’ and the pressure has no ‘elevation because of anxiety’ component. Smart physicians, in any case, discount the recorded pressure a bit because of the ‘white coat’ effect.
Measuring blood pressure: The physician ties his Sphygmomanometer cuff just above your left elbow – the level of your heart, for accuracy. In reality it can be done anywhere on the body when necessary. The tight grip of the cuff ensures that the air pressure in the cuff ‘balances’ the pressure of the blood in the blood vessels below your skin. The first time can be scary with the vice-like grip of the cuff and the doctor usually takes a couple of more readings when you are supposedly ‘relaxed’ and the pressure has no ‘elevation because of anxiety’ component. Smart physicians, in any case, discount the recorded pressure a bit because of the ‘white coat’ effect.
(We Trivedi’s routinely do it ourselves on a digital instrument and have developed understanding about what those numbers show. It is amazingly empowering. With reduced salt intake, smart food, intelligent oil consumption, physical activity, positive attitude bolstered by strong family bonds, tracking of BP and BMI, interpretation of deviations and readiness to consult the physician in case of suspicion, we have virtually eliminated the possibilities of catastrophic events.)


The physician pressurizes his meter above the systolic pressure stopping the blood flow downstream of the cuff. He then very slowly releases the air reducing its pressure in the cuff which has the effect of reducing the restriction on the blood flow. He listens intently for the exact balance between the air pressure and the systolic pressure with impending re-start of blood flow as the indicator. That air pressure is the systolic blood pressure.
As he reduces the pressure further, the blood begins to flow past the artificial external constriction with the blood pressure decreasing. Listening intently, he looks out for another ‘balance’ when the relaxing blood pressure is balanced by the air pressure in the cuff. Having so measured the diastolic pressure, he quickly empties out all air, removes the cuff and somberly declares something like, “135/83.”
Not bad at 50+. Offers advice on the lines of what we Trivedi’s do. Asks if either parent had hypertension or diabetes or obesity and what it led to. If he recommends electrocardiogram, echo-cardiogram, treadmill test or even angioplasty, do not cringe. He means well and wants you to exploit the miracles of modern medicine and we want you to let food lift life.
Hypertension: While blood without pressure is of no use, elevated arterial pressure is the beginning of all sorts of trouble. It is ‘hypertension’ – defined as systolic pressure above 140 mm Hg or diastolic pressure above 90 mm Hg. ‘Normal’ blood pressure depends upon so many factors that you would be forgiven for giving up on knowing. But 120/80 are good numbers, (even lower in healthy youngsters) though difficult to maintain!
As we age, the blood vessels lose some of their flexibility with the result that blood pressure gradually increases as the blood vessel walls do not ‘accommodate’ the pressure by expanding fully and ‘resist’ the pressure. This is the well-known ‘hardening’ of the arteries – age-related. The aforesaid ‘fatty deposits’ on the walls of the vessels also have practically the same effect. Both together are obviously, bad.
Origin of hypertension: This is an intricate cardiological problem with origins so varied, it includes endocrinology (hormones), gynaecology, nephrology (kidney microstructure and functioning), neurology, haematology (blood composition and its distortions), general physiology and psychology as well. In continuation of our CAD-CHD theme, here we will focus only on fatty plaque and age related conditions – by far the commonest and nature’s favorite. But for simplified essentialness, it is useful to see hypertension as:
- Heart’s compulsive ‘higher frequency and/or higher amplitude beating or pulsations’ making blood flow out with urgency. (Typically, this happens when you exercise or are suddenly anxious etc). Note: frequency is the heartbeats per minute and amplitude is the extent of contractions and expansions at every beat.
- ‘Resistance to blood flow’ because of age-related and/or obstructive hardening of arteries. (Ref previous two posts). Obviously, the bp downstream of the obstruction is less than upstream (which is raised) and struggles to maintain a flow rate that will not hamper oxygen and nutrition supply. (Ref post no. 25). Such flow resistance can sometimes be ‘organic’. For example, the filtering microstructures in the kidneys (nephrons) filter out watery waste (urine) under the systolic blood pressure. Their malfunction (like the clogged tea strainer) can increase the pressure of the blood reaching them which is essentially the systolic pressure.
Also note: hypertension originating elsewhere (e.g. atherosclerosis) can damage delicate nephrons and increase their resistance setting off a disastrous spiral. Please keep life as clean and simple as you can; it is difficult to clean up afterwards. In simple language, this is known as ‘prevention is better than cure’. Let only the inevitable complications happen; don’t add your own. And let food lift life!
Effects of hypertension: Mainly,
- It erodes (rubs hard) the arteries exposing them to the risk of injury. This can potentially initiate arterial plaques (ref the previous post)
- It strains the heart risking its longevity.
- Coronary occlusion with myocardial infarction (Ref the previous post) is a special case in which, throttled blood supply reducing oxygen and nutrient availability to the heart wall is the pronounced effect. Elsewhere, hypertension affects all organs e.g. kidneys and brain which have delicate and intricate internal structures carrying pressurized blood in extremely delicate capillaries. These blood vessels – not very far from the heart – take the brunt of increased blood pressure in the aorta.
- It can cause rupture of minute vessels causing internal haemorrhages. Brain haemorrhage is a common example.
Next Post:
Diabetes – the creeping, corrosive curse
But food, lifestyle and even attitude can help!
Visit Disclaimer
4 thoughts on “Blood pressure and hypertension – Their nature, origin, effects and remedies with focus on food”
Hi there! This post couldn’t be written any better! Reading through this post reminds me of my previous room mate! He always kept talking about this. I will forward this article to him. Pretty sure he will have a good read. Thank you for sharing!
Valuable info. Lucky me I found your site unintentionally, and I am shocked why this accident did not happened in advance! I bookmarked it.
Thought-provoking
Very detailed